Serving our community since 2004, Friendship Circle of Miami offers a wide range of social and recreational programs for adults ages 18+ that are tailored to their individual abilities. Our unique programs are designed to help participants acquire new skills while creating meaningful and lasting friendships with their peers.
Step into
our Circle and experience the Magic of Friendship!

Social Group for Adults
This circle is a great opportunity for adults with special needs to come together, hang out, and enjoy the company of friends and adult volunteers. Our social group has FUN while helping to build social skills. Participants will enjoy fun and engaging activities and experiences through gatherings that take place both on and off-campus.
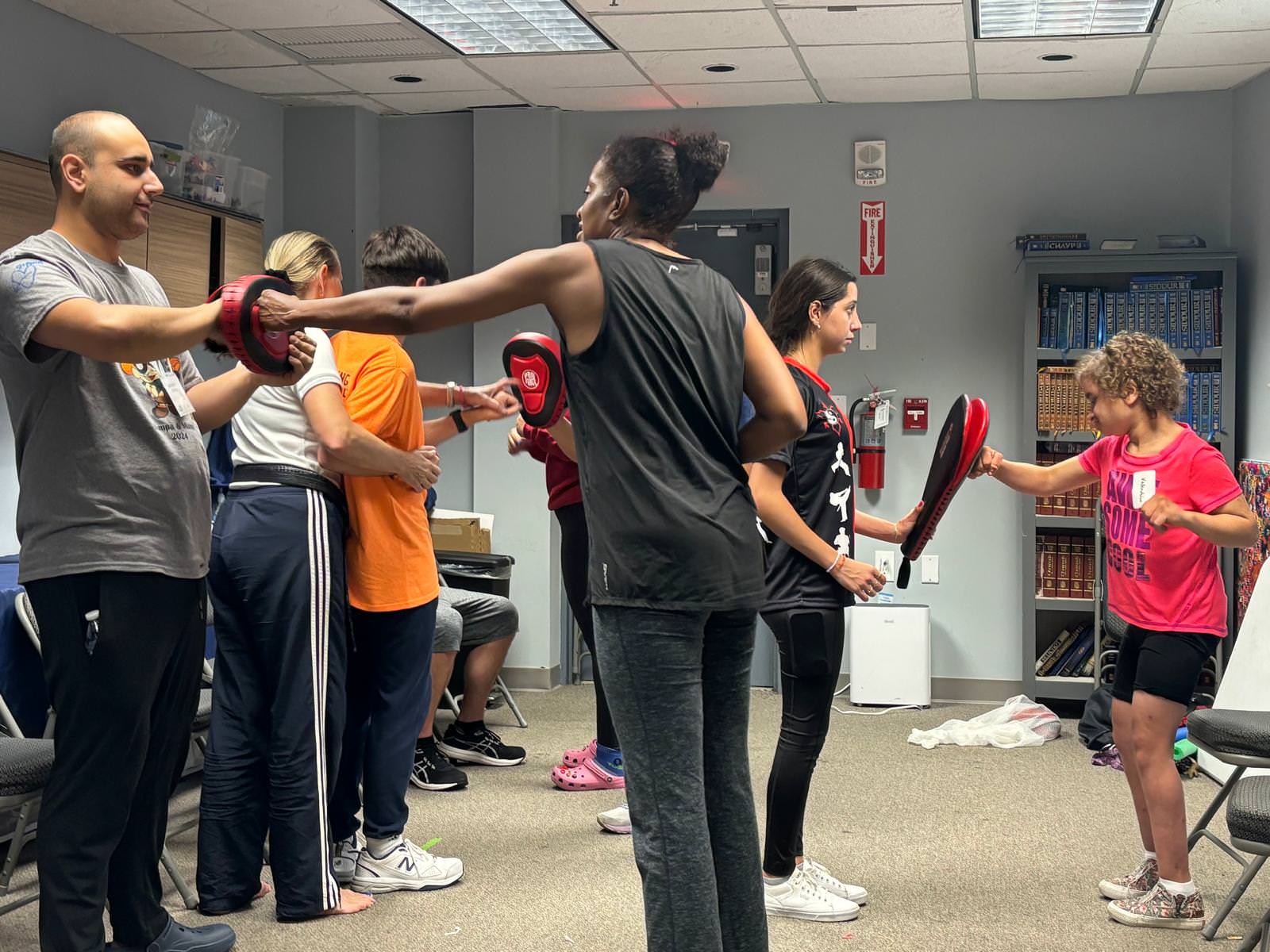
Karate Circle
Karate is a way to let loose and have some fun! Teaching our budding martial artists to practice in a safe, controlled environment with trusted teachers. Participants will learn all the basic punches, kicks, stances, and blocks.

Art Circle
Unlock your creativity! Participants will learn various art techniques and be exposed to many different mediums under the artistic direction of our fabulous instructors and with the support of our dedicated volunteers.
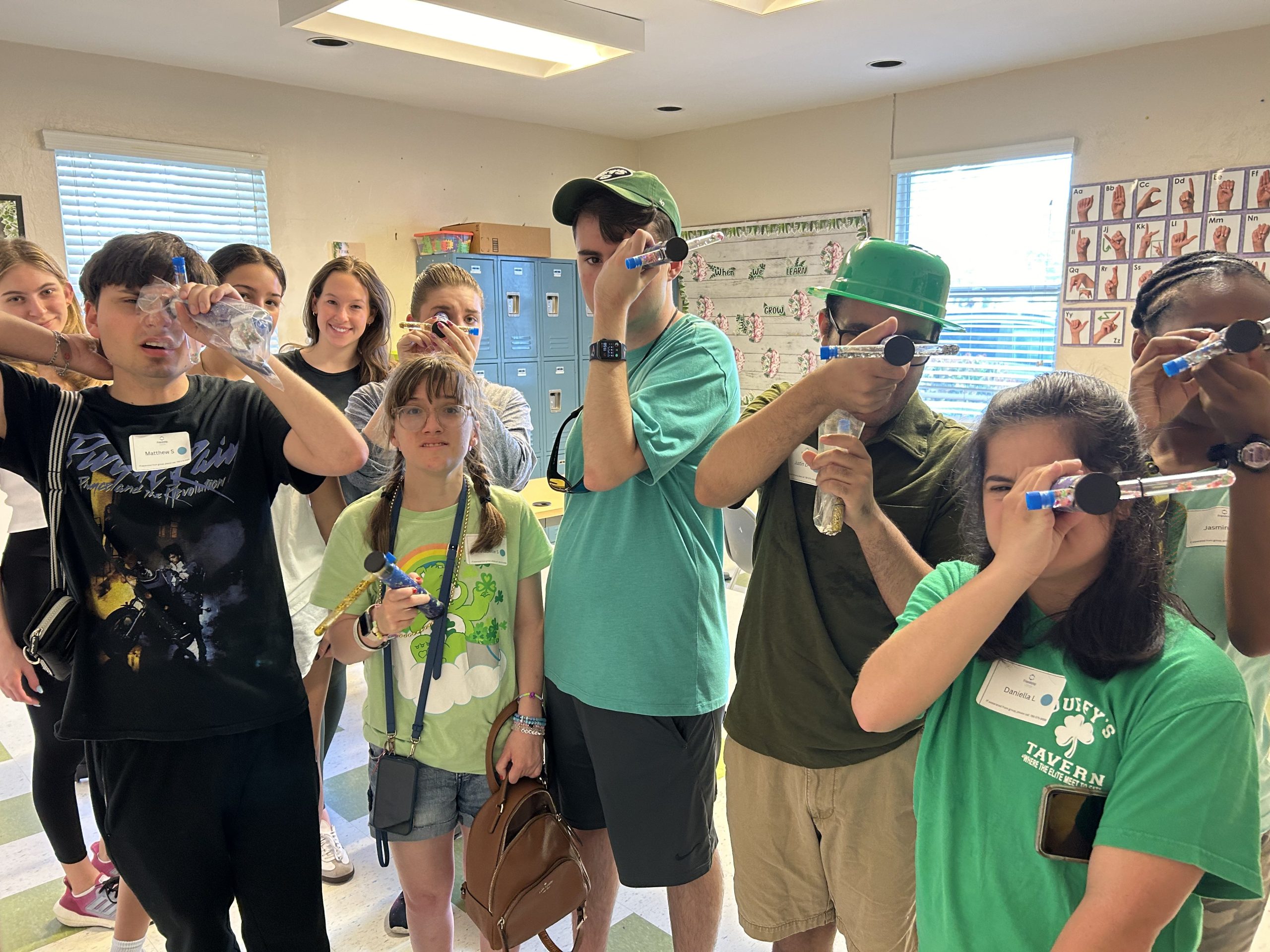
Sunday Circle
This is our Sunday drop-off program that serves children and adults ages 5-22 years old two Sunday’s a month. This program offers music therapy, karate, dance, Zumba, science, art and crafts, and much more! Every Sunday is something new! The sessions are led by credentialed instructors and therapists with dedicated volunteers to assist each participant.
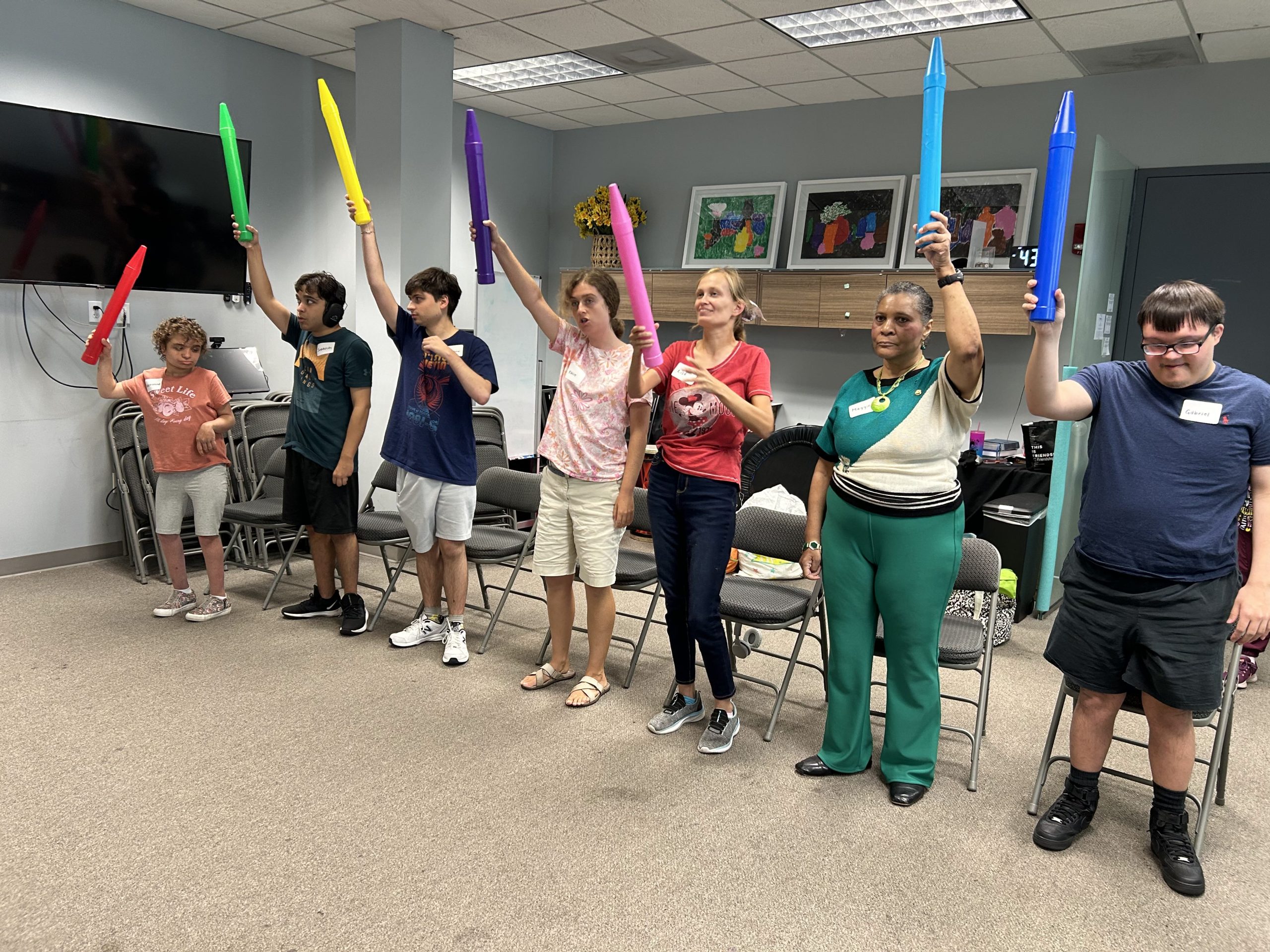
Movement Mondays
Participants of all ages will join in an engaging and high energy Zumba and Hip Hop program that provides opportunities to enjoy fun and friendship under the direction of our amazing instructor!
Friendship Circle Band
One of our top attended programs, our participants learn and jam out on the keyboard, guitar, drums, and other instruments with friends! Participants and volunteers perform at public functions together, showcasing their talents and friendships.


Spring/Summer/Winter Camp
Participants aged 5 to 22 will never get bored during break again! Get ready for excitement and FUN with awesome field trips to the water park, museum, zoo, arcades, bowling, and so much more!
No School Fun Days!
Participants aged 5 to 22 enjoy a break from school with an action-packed day of fun and thrills for Veteran’s Day, Martin Luther King Jr. Day, and President’s Day. While everyone is out of school, we are having FUN!
